Stat | Lytes | Drugs | ID | Heart | Lungs | Kidneys | GI | Rheum | Heme-Onc | Endo | Neuro | Derm | Misc. | Resource | Home
VERTIGO See also vestibularneuritis.htm | BPV.mht | BPV2009.mht
![]() E-Note for Adult
Medicine
E-Note for Adult
Medicine
Stat | Lytes |
Drugs | ID |
Heart | Lungs |
Kidneys | GI |
Rheum | Heme-Onc |
Endo | Neuro |
Derm | Misc. |
Resource |
Home
VERTIGO
See
also vestibularneuritis.htm |
BPV.mht |
BPV2009.mht
Benign positional vertigo (BPV) is the most common cause of vertigo.
Vertigo is an illusion of motion (an illusion is a misperception of a real
stimulus) and represents a disorder of the vestibular proprioceptive system.
VERTIGO IS A HALLUCINATION OF SELF- OR ENVIRONMENTAL MOVEMENT,
MOST COMMONLY A FEELING OF SPINNING, USUALLY DUE TO A DISTURBANCE IN THE
VESTIBULAR SYSTEM.
Differentiation of Peripheral and Central vertigo:
Sx |
Peripheral (labyrinth) |
Central (brainstem or cerebellum) |
| Tinnitus/deafness | Often present | Usually absent |
| Assoc.central abnormallity | None | Extremely common |
| Severity of vertigo | Marked | Usually mild |
| Nystagmus: Direction |
Unidirectional; fast phase -opposite lesion |
Bidirectional or uni- |
| Purely horizontal nystagmus component |
Uncommon | Common without torsional |
| Vertical or purely torsional component |
Never present | May be present |
| Visual Fixation | Inhibits nystagmus/vertigo | No inhibition |
| Common Causes | Infectious labyrhintitis, Meniere's, neuronitis, toxin, ischemia, trauma |
Vascular, demyelinating, neoplasm |
| Duration of Sx | Finite(min to wks),may recur | May be chronic |
The standard test for vestibular function is ENG (Electronystagmography), where warm & cold water is applied to the tympanic membranes, & the nystagmus pattern is studied.
A. VERTIGO:
B. Presyncope / Syncope
C. Dysequilibrium
D. Mental Status Changes
E. Psychiatric Disease (~20%)
Differential Diagnoses of Benign paroxysmal positional vertigo (BPPV)
Other Problems to Be Considered in BPPV
The Dix-Hallpike Testing Maneuver picture | Video of the Maneuver
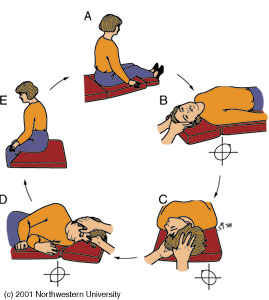
The modified Epley Maneuver picture
![]()
![]()
RX of acute vertigo:
bedrest & vestibular suppressant drugs as: meclizine, dimenhydrinate,
promethazine, scopolamine, diazepam.
If the Sx persists beyond a few days, most authorities advise ambulation in an attempt to induce central compensatory mechanisms, despite the short-term discomfort to the pt.
Chronic vertigo of labyrinthine origin may be treated with a systematized exercise program to faciliate compensation.
Differential Diagnosis of Acute Vertigo:
Labyrinthine vertigo:
Vestibular Vertigo (vestibular nerve origin):
Vestibular neuronitis & benign recurrent vertigo (unknown cause):
RX: as in Meniere's Disease.
Acute unilateral labyrinthine dysfunction is idiopathic, or caused by infection, trauma, & ischemia.
Acute bilateral labyrinthine dysfunction is usually the result of toxins, drugs or alcohol.
Acoustic neuroma (The eight cranial nerve Schwannomas) grows slowly & produce such a gradual reduction of labyrinthine output that central compensatory mechanisms prevent or minimize the vertigo; auditory Sx of hearing loss & tinnitus are the most common Sx.
Recurrent unilateral labyrinthine dysfunction with cochlear disease (tinnitus/deafness) is usually due to Meniere's disease.
Recurrent unilateral labyrinthine dysfunction without auditory Sx is called vestibular neuronitis.
TIA of posterior cerebral circulation (vertebrobasilar insufficiency) almost never cause recurrent vertigo without concomitant motor, sensory, visual, cranial nerve, or cerebellar signs.
Positional vertigo is precipitated by a recumbent head position (not just the head movement), either to the right or to the left.
Benign paroxysmal positional vertigo (BPPV) is particularly common. It generally abates spontaneously after weeks or months. Its nystagmus pattern is distinctive. The lower eye displays a large-amplitude torsional nystagmus, & the upper eye has a lesser degree of torsion combined with upbeating nystagmus. If the eyes are directed to the upper ear, the vertical nystagmus in the upper eye increases in amplitude.
Psychogenic vertigo, usually a concomitant of agoraphobia (fear of large open spaces, crowds, or leaving the safety of home) should be suspected in pts so "incapacitated' by their Sx that they adopt a prolonged housebound status. It has no nystagmus during a vertiginous episode.
MENIERE'S DISEASE OR SYNDROME:
Recurrent vertigo associated with tinnitus & progressive deafness.
The pathological changes are said to consist of a dilatation of the endolymphatic
system which leads to a degeration of the delicate bestibular & cochlear
hair cells.
RX:
During acute attack, rest in bed is the most effective Rx.
Meclizine, demenhydrinate, cyclizine 25-50 mg tid is useful in treating more
protracted attacks.
Mild sedative drugs may help the anxious pt between attacks.
Usually the deafness is unilateral & progressive, & when it is complete,
the vertiginous sttacks cease. However, the course is variable.
BENIGN POSITIONAL VERTIGO
Occurence of paroxysmal vertigo & nystagmus with the assumption of certain
critical positions of the head, secondary to labyrinthine dysfunction.
RX:
REF: Harrison 1994
REVIEW - Primary Care: Benign Paroxysmal Positional
Vertigo - J. M. Furman and S. P. Cass
NEJM Volume 341, Number 21: November 18, 1999
Motion
Sickness [Paul M. Gahlinger, MD VOL 106 / NO 4 / OCTOBER
1, 1999 / POSTGRADUATE MEDICINE]
Dizziness among Older Adults: A Possible Geriatric Syndrome - Mary
Tinetti
Annals
of Internal Medicine, 7 March 2000. 132:337-44.
Maneuvers for benign positional vertigo
VOL 105 / NO 5 / MAY 1, 1999 / POSTGRADUATE MEDICINE
Q: Do the maneuvers I've heard about to treat benign positional vertigo really work? How are they performed? Can patients be taught to do them at home? Epley's Particle-repositioning maneuver: The modified Epley Maneuver picture
A: Benign paroxysmal positional vertigo is a self-limited vestibular disorder characterized by vertigo and nystagmus that are provoked by a change in position. Pathophysiology entails displacement of otoconia (calcium carbonate crystals) that are normally adherent to the utricle and saccule within the vestibule. These particles can float to the dependent portion of the posterior semicircular canal and become lodged. Head movements (eg, neck hyperextension or supine positioning toward the involved ear) cause the particles to move, due to gravitational forces, and induce flow of inner ear endolymph. This stimulates the inner ear, creating the sensation of vertigo with associated upward and rotary nystagmus.
In the particle-repositioning maneuver, described by Epley,1 the patient is rapidly placed into the provocative supine position. The patient's neck is hyperextended, and he or she is rolled 270° toward the contralateral ear until the face-down position is reached. The maneuver is done over a 2-minute period, often with the assistance of a vibrator positioned over the involved temporal bone. The patient is then returned to a sitting position. Patients are instructed to avoid lying flat, hyperextending the neck, or bending over for the following 36 hours.
This maneuver is remarkably successful in most cases. In about one third of patients, symptoms recur after a few years, but patients can learn to do the maneuver at home and repeat it as necessary.
Vestibular-rehabilitation exercises have been successful in achieving relief of symptoms by habituation in patients who do not respond to the maneuver.
References
Epley JM. The canalith repositioning procedure: for treatment of benign
paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107(3):399-404
Barry E. Hirsch, MD Associate Professor Department of Otolaryngology, University of Pittsburgh School of Medicine
See also Mayo Clin Proc July 2000;75:695 - David Froehling, etc The Canalith Repositiong Procedure
The dizzy patient - Presence of vertigo points to
vestibular cause - Robert W. Baloh (UCLA)
VOL
105 / NO 2 / FEBRUARY 1999 / POSTGRADUATE MEDICINE
Decision Making in Medicine: Dizzy Patients: The
Varieties of Vertigo -Robert W. Baloh (UCLA)
Hosp Pract 1998
June
03142003
![]()
![]()
{kind=link}
{kind=link}
{kind=link}