Percutaneous Endoscopic Gastrostomy (PEG) Tube Feeding
|
| REF:
|
What is percutaneous
endoscopic gastrostomy (PEG)?
-
Percutaneous endoscopic gastrostomy (PEG) is a surgical procedure for placing
a feeding tube without having to perform an open operation on the abdomen
(laparotomy). A gastrostomy (a surgical opening into the stomach) is made
percutaneously (through the skin) using an endoscope (a flexible, lighted
instrument) to determine where to place the feeding tube in the stomach and
secure it in place.
|
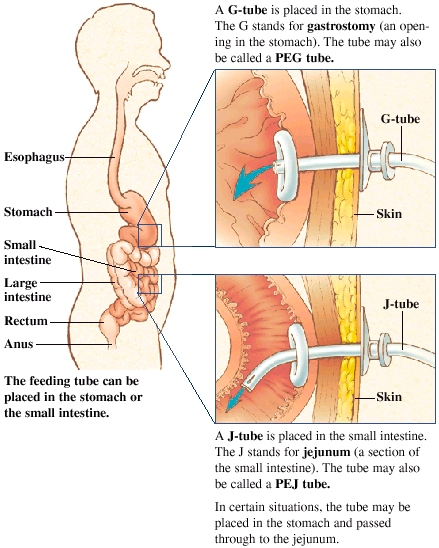
| Picture of PEG Tube Feeding
|
What is the purpose
of PEG?
-
The aim of PEG is to feed those who cannot swallow. Irrespective of the age
of the patient or their medical condition, the purpose of PEG is to provide
fluids and nutrition safely and directly into the stomach, to significantly
increase the quality of life, maintaining appropriate weight levels and
nutritional requirements.
|
|
Who does
PEG?
-
PEG is done by a doctor. The doctor may be a general surgeon, an otolaryngologist
(ENT specialist), a gastroenterologist (GI specialist), etc.

 |
|
Where is PEG
done?
-
PEP is performed in a hospital or outpatient surgical facility.
|
|
How is PEG
done?
-
PEG tubes are placed with the aid of an endoscope (a flexible, lighted
instrument), the scope going down the throat (with local anesthesia to the
throat) to assist in guiding the placement of the tube through the wall of
the stomach. The surgery is simple and involves little risk or discomfort.
The procedure takes about 20 minutes. The doctor then makes a small incision
(cut) in the skin of the abdomen and pushes an intravenous cannula (an IV
tube) through the skin into the stomach and sutures (ties) it in place. The
PEG tube extends from the interior of the stomach to outside the body through
a small incision only slightly larger than the tube itself in the abdominal
wall. The tube is prevented from coming out of the stomach by one of several
methods. Some brands have a small wire within the tube, which after insertion
is pulled from the exterior end of the tubing causing the portion within
the stomach to curl up or “pigtail,” preventing it from being pulled
out. Other systems employ a very small balloon at the end of the tube which
is inflated within the stomach after insertion, serving the same purpose.
Removal of the tube simple involves cutting the wire which created the pigtail,
or deflating the balloon section of the tube allowing it to slip easily from
the stomach. About three inches of tubing will protrude from the incision
area. Initially, there may be some discomfort while getting used to using
the system, from gas or air, or from adjusting to the liquid foods themselves.
|
|
When can the
PEG patient go home?
-
The patient can usually go home the same day or the next morning.
|
|
What are the
possible complications with PEG?
-
Possible complications include wound infection (as in any kind of surgery)
and dislodging or malfunction of the tube.
-
The likelihood of complilcations may occur but is slight, with only a one
percent chance of major problems (gastric hemorrhage, peristomal leakage)
and an eight percent chance of minor ones (infection, stomal leaks, tube
extrusion or migration, aspiration and fistula formation). Aspiration
is perhaps the most common complication related to tube feeding. This
occurs when food is actually inhaled into the lungs. Aspiration can lead
to pneumonia, but if the patient is kept upright during feeding, the likelihood
of developing this complication can be greatly minimized.
|
|
Major
complications include:
-
Aspiration pneumonia
-
Gastric perforation
-
Gastrocolic fistula
-
Internal leakage
-
Dehiscence
-
Peritonitis
-
Subcutaneous abscess
-
Buried bumper syndrome (migration of the internal bumper of the PEG tube
into the gastric or abdominal wall).
Minor complications include:
-
Tube problems:
-
Tube blockages
-
Tube dislodgements
-
Tube degradation
-
External leakage
-
Unplanned removal
-
Site infections (common but rarely serious.12 There have been studies to
determine whether prophylactic antibiotics prevent such infections.
Call Your Doctor If Any of the Following
Occurs
-
Signs of infection, including fever and chills
-
Redness, swelling, increasing pain, excessive bleeding, or discharge from
the incision site
-
Headaches, muscle aches, dizziness, fever, or general ill feeling
-
Nausea, constipation, or abdominal swelling
-
Vomiting
|
|
|
|
|
|
|
|
|
|
| G |
|
{kind=link}