 TOC |
Rheumatology
TOC |
Rheumatology

Approach to Knee Pain
REF: Painful Knee Test
2008
Strategy I.
Separate all knee pain patients into one of three categories:
-
Routine office visit knee pain
-
The hot swollen atraumatic knee -
need knee tap
Septic arthritis
Gout, pseudogout
Autoimmune-inflammatory
-
Acute knee injury: the blow
out --> See the Examination
& the Referral Decisions for acutely
injured knee below!
Strategy II.
Analyze the location
of the most painful part of knee
in all routine office visit knee pain complaints
Anterior - Medial - Lateral - Posterior Knee Areas
| Anteriorly
|
Medially
-
Meniscal tear or cyst
Symptoms of meniscal pathology: pain, swelling, locking with flexion,
giving way
Signs: medial joint line tenderness, effusion/synovitis, locked
knee, atrophy, loss of full extension or flexion
-
Osteoarthritis
History: older age, activity trauma, surgery, effusions, pain
P/E: joint line tenderness, varus, crepitation, effusion, Pain at extreme
motion
X-ray: narrowing, osteophytes, sclerosis, cysts
Rx: bicycling, PT Rx, NSAID, chondroitin & glucosamine, activity
modification, steroid injection, surgery, ? hyaluronate injection?
-
Osteochondritis dissecans (rare)
Cause unknown, may be avascular necrosis of bone or femoral condyle
Teenage boys ? girls 10:1
Pain, swelling +/- locking, effusion, atrophy, tenderness, 1 year course
Knee X-ray of Tunnel View
Refer to Ortho for persistent pain, effusion, or locking
Rx: activity modification _/- arthroscopy
-
Osteonecrosis of the femoral condyle (rare)
Older age group > 60 yo with sudden severe pain while walking
("spontaneous")
Pain unrelenting, tumor like , unresponsive to usual Osteoarthritis Rx
Initial X-ray negative, Tunnel View x-ray positive, later MRI shows avascular
necrosis (AVN)
Crutches, steroids, bike exercise, may need TKR (Total Knee Replacement)
|
Laterally
-
Meniscal tear, cyst, discoid
Meniscal Cyst (Lateral > Medial) is the mucinous degeneration in a meniscus
that produces a mass over or near lateral joint line. Never a tumor.
Ignore if possible. Aspirate if requested x1. Definitive Rx includes
a menisectomy, so treat by benign neglect if possible.
Symptoms of meniscal pathology: pain, swelling, locking with flexion,
giving way
Signs: join line tenderness, effusion/synovitis, locked knee, atrophy, loss
of full extension or flexion
-
Osteoarthritis
-
Ilio-Tibio-"Band" Fascia Friction syndrome
Usually sports related, high arches, the only cause of pain & tenderness
above lateral joint line!
Rx: stretch ITB, warm up, ice, NSAID, steroid injections last resort.
-
Biceps tendinitis
Activity related, tender tendon at posterolateral side of knee above fibular
head.
|
Posteriorly
-
Knee Effusion of any cause
Large amount of synovial fluid commonly produces tightness, fullness, or
discomfort in back of knee.
Rx the cause of effusion.
-
Baker's cyst
Usually due to the herniation of fibrosynovial knee tissue into the popliteal
fossa due to intra-articular disease. Always benign, best ignored.
Aspirate x1 only if needed to prove diagnosis.
-
Sciatica
May cause pain behind knee from radiculopathy or hamstring spasm. A
pseudo-flexion contracture may be present.
 |
Strategy III. ** Consider Timely Orthopedic
Referral for the following patients:
-
Recurrent effusion
(in otherwise "healthy"
knee)
-
Giving way
(with strong quadriceps muscle)
- torn meniscus
- loose body
- patella subluxation
- ligamentous instability
-
Locking of the knee
(not pseudo-locking)
- torn meniscus
- loose body
- osteoarthritis
- pseudolocking
-
Definite loud pop at time of
injury
- Anterior Cruciate Ligament ACL Tear
- Meniscus Tear
- Dislocated patella
- Torn MCL
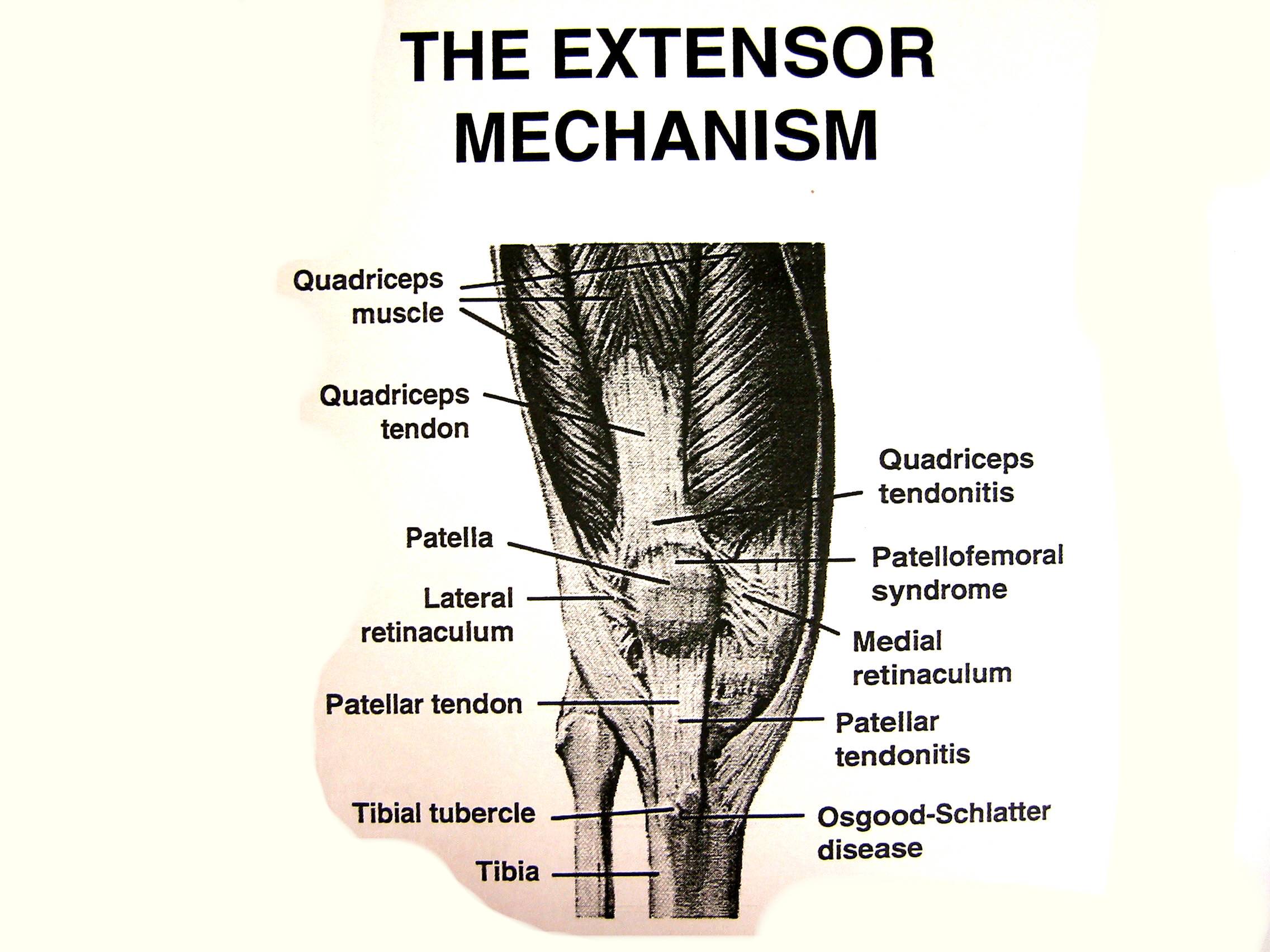
Patello-femoral Pain
Syndrome
Symptoms of Patello-femoral Pain Syndrome
-
Anterior knee pain
-
Popping & clicking
-
Instability - Giving Way
-
Pseudo-locking
-
Pain after sitting (movie sign)
-
Pain ascending stairs
-
Effusion & "swelling" are not usual
-
The patellar pain are aggravated by flexed knee activities as sitting, climbing,
squatting
Physical Findings in Patello-femoral Pain Syndrome
-
Muscle contractures
-
Quadriceps atrophy
-
Q-Angle increased
-
Foot alignment (pronation)
-
Apprehension Sign (in dislocators)
-
Effusion, heat are not typical
Conservative Rx of Patello-femoral Pain Syndrome
-
Stretching
-
Strengthening
-
Orthotics
-
Soft goods
-
Activity modification
-
NSAID as analgesics
Surgical Rx of Patello-femoral Pain Syndrome
-
Soft Tissue:
-
Lateral release
-
Proximal realignment
-
Distal realignment
-
Bone Tissue:
-
Distal realignment
-
Tibial tubercle osteotomy
-
Chondroplasty
-
Patellectomy
Prepatellar Bursitis
("Housemaid's Knee") : Sterile bursitis
-
vs septic bursitis (abscess &
cellulitis) which looks awful with moderate pain.
-
Rx of septic bursitis: aspirate or I/D, culture & sensitivity, antibiotics
Rx
Patellar Tendinitis
("Jumper's Knee")
-
Pain & tenderness in tendon below patella
-
Rx: warm up, stretch, NSAID, ice, activity modification, brace.
Quadriceps
Tendinitis
-
Pain & tenderness above patella, ma lead to rupture
-
Rx: stretch, strengthen, activity modification, etc.
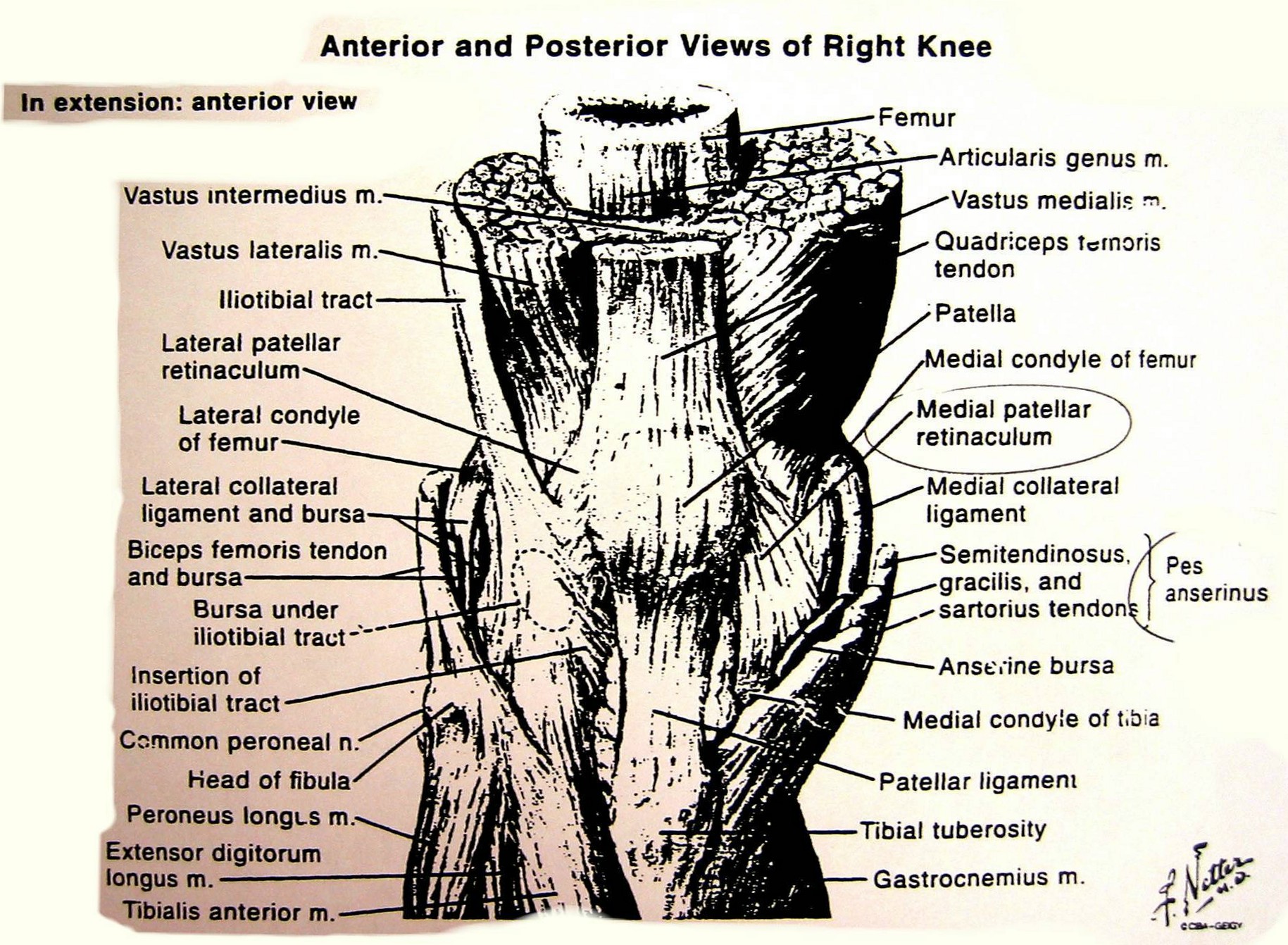
Pes Anserinus Bursitis/
Tendinitis
-
Pain, tenderness, & swelling below medial joint line anteriorly
-
Differential Dx: stress fracture of tibia
Plica Syndrome
-
Overly diagnosed, normal fibrosynovial fold in knee
-
Rarely a cause of knee pain except after a direct blow
Chondromalacia patella
-
It is age related & usually asymptomatic
-
It should be rejected as a clinical diagnosis
-
The identical clinical syndrome can occur when the articular cartilage has
a normal appearance (Insall 1982)
Osgood-Schlatter Disease:
-
Traction apophysitis, esp. in teenage boys.
-
Tender & swollen over tibial tubercle
-
Rx: activity modification (rest, no jumping), stretch, strengthen, ice
General Treatment of Painful Knees:
Bicycling!
-
Strengthens muscles
-
Aerobic fitness decreased chronic pain
-
Weight control
-
Mechanical smoothing
-
Stimulates some healing in cartilage
Others:
-
Stretch & strengthen
-
NSAID
-
Activity modification
-
Steroid injections
-
Softwear
The Examination of
The Acutely Injured Knee
* Must get knee x-ray for all acute injured knee to rule out fracture
or loose bodies.
The Critical Questions (History)
-
1st time or recurrent problem, has it happened before?
-
Loud "POP" at time of injury (Anterior Cruciate Ligament Tear?)
-
Timing of swelling (SLOW - effusion; FAST - hemarthrosis)
-
Can pt continue the activity/sport or not
Six Steps to Evaluating The Acutely Injured
Knee:
-
Support the painful knee with a support ("a can") to keep the flexion
about 20o
-
Check for knee effusion vs hemarthrosis
-
Check for Range of Motion assisted: Is the knee locked, cannot
extend of flex over 90o
-
Examine the Patella for stability & retinacular tenderness
- Apprehension Sign (Fairbank's Test) - move Patella laterally
- Medial patellar Retinacular tenderness
- Hemarthrosis
-
Examine the Ligaments (R/O Tear) by palpation & stress
maneuver
- MCL (Medial Collateral Ligament): palpate & stress it
- ACL (Anterior Cruciate Ligament): Lachman's test & pivot shift
- LCL (Lateral Collateral Ligament): palpate & stress it
- PCL (Posterior Cruciate Ligament): Sag sign
-
Examine the Extensor mechanism: integrity versus disruption
- active extension possible?
- palpate patellar tendon for defect (rupture)
- palpate quadriceps tendon for defect (rupture)
- compare location of right & left patellae
Initial Treatment of Sprained Knee (Except displaced
fractures)
-
Aspiration rarely needed
-
Minor: RICE (rest, ice, compression, elevation); crutches, partial
weight bearing
-
Major: large compressive bandate "Jones", splint slightly flexed, crutches,
analgesics (NSAID)
Referral Decisions
for The Acutely Injured Knee:
Immediate Orthopedic Consultation for:
-
All fractures
-
Quadriceps Tendon Tear
-
Patellar Tendon Tear
-
Dislocated unreduced Patella
-
Locked Knee
Early (within 1 week) Orthopedic Consultation
for:
-
Acute ACL/PCL (Anterior/Posterior Cruciate Ligament) Tears
-
Grade 3 MCL/LCL (Medial/Lateral Collateral Ligament) Tears
-
Acute Patellar Dislocation
Elective Orthopedic Consultation for:
-
Recurrent Patellar Dislocation
-
Chronic ACL/PCL Tears
05072003 Most of the written material from
the Knee Workshop by Dr. Barry J. Miller 2003