Hypogonadism
Hypogonadism REF: Cecil Texbook of Medicine 2006 | Ferri's Clinical Advisor: Instant Diagnosis and Treatment 2006 | UpToDate 2006 |
Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | hypogonadism2008.pdf |
| Hypogonadism in a man refers to
a decrease in either of the two major functions of the testes:
sperm production and testosterone
production. Diminished testosterone secretion during adulthood leads to decreases in energy, libido, sexual hair, muscle mass, and bone mineral density, & possible erectile dysfunction. These abnormalities usually result from
In occasional cases, however, a defect in the ability to respond to testosterone is the cause of hypogonadism. Primary hypogonadism is more common than secondary hypogonadism and differs in two characteristics:
Secondary hypogonadism is less common than primary hypogonadism and differs in two characteristics:
|
| Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | |
| PRIMARY
HYPOGONADISM (TESTICULAR HYPOGONADISM) Primary hypogonadism refers to a condition of androgen deficiency with or without infertility in which the pathologic process lies at the testis level. - Decreased Testosterone & sperm count, Increased LH or FSH |
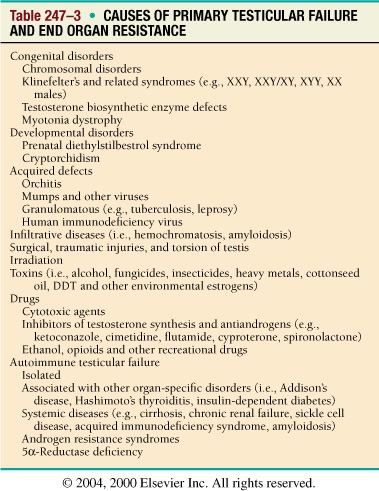
Causes of Primary Testicular Failure & End Organ Resistance I. Congenital Abnormalities:
II. Acquired defects or
diseases:
|
| Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | |
| SECONDARY HYPOGONADISM (HYPOGONADOTROPIC HYPOGONADISM)
a deficiency in the secretion of gonadotropins (LH and FSH) due to an intrinsic or functional abnormality in the hypothalamus or pituitary glands. - Decreased Testosterone & sperm count, Normal or Decreased LH or FSH |
| Such disorders result in the secondary
Leydig cell dysfunction . The clinical manifestations depend on the
age of the patient at the onset of the disorder.
Hypothalamic-Pituitary Disorders (Secondary Hypogonadism)
Causes of Secondary Gonadal Insufficiency (Hypo-gonadotropic Hypogonadism) - detail see the section below.
Causes of Secondary hypogonadism
I. CONGENITAL
ABNORMALITIES
II. ACQUIRED DISEASES
In general, a mass lesion in the pituitary or hypothalamus is more likely to diminish the secretion of gonadotropins than that of ACTH and TSH. Thus, patients may present with hypogonadism without either adrenal or thyroid deficiency.
|
| ANDROGEN RESISTANCE
(ANDROGEN-SENSITIVE END ORGAN DEFICIENCY) Certain conditions have clinical phenotypes mimicking testosterone deficiency in the absence of lowered testosterone levels. These are either drug induced (antiandrogens) or congenital defects in the androgen receptor, postreceptor defects, or 5a-reductase deficiency Defects in Androgen Action
* From Andreoli TE (ed): Cecil essentials of medicine, ed 4, Philadelphia, 1997, WB Saunders. Lab. Evaluation:
|
Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | |
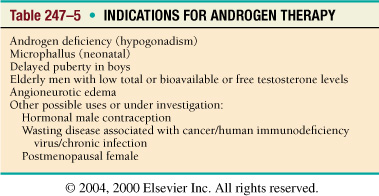
TREATMENT OF TESTOSTERONE / ANDROGEN DEFICIENCY INDICATIONS:
The principal goal of testosterone therapy is to restore the serum testosterone concentration to the normal range. The most available and commonly used blood measurement of testosterone is serum total testosterone. The normal range of a young adult male population varies for different laboratories but should be in the general range of 300 to 1000 ng/dL (10 to 38 nmol/L). Total testosterone measurements may be misleading indicators of Leydig cell status in conditions in which SHBG levels are abnormal (see earlier section). Under these circumstances, a measurement of free testosterone (by dialysis method), bioavailable testosterone (free + albumin bound), or calculated free testosterone (utilizing total testosterone and SHBG measurements) is useful to characterize circulating bioactive testosterone levels. The following rules apply to most young and middle-aged men suspected of hypogonadism.
Thus, when serum total testosterone is borderline and LH is not increased, measurement of one of the bioactive testosterone level levels is indicated. The guidelines for men over the age of 60 years are less certain; since SHBG levels are increased in this age group, total testosterone levels may overestimate the biologically active forms of circulating testosterone. In men older than 60 years with signs and/or symptoms of androgen deficiency, a serum total testosterone level greater than 400 ng/dL argues strongly against hypogonadism; a serum level less than 200 ng/dL is almost always a clinically significant level, and total testosterone concentrations between 200 and 400 ng/dL deserve further testing with one of the tests of bioactive testosterone. Indications for Testosterone/Androgen Therapy
CONTRAINDICATIONS TO TESTOSTERONE THERAPY:
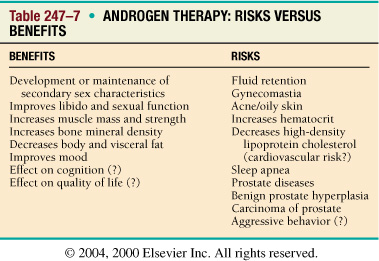
BENEFITS VERSUS RISKS OF ANDROGEN THERAPY: Table 247-7 shows the benefits and potential side effects of androgen treatment. In hypogonadal men, androgen replacement leads to the development and maintenance of secondary sexual characteristics. Testosterone has important anabolic effects on muscle and bone and improves libido and sexual dysfunction. It has less effect on erectile dysfunction (see later section on sexual dysfunction). Benefits of Testosterone/Androgen Therapy
Risks of Testosterone/Androgen Therapy
|
| Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | |
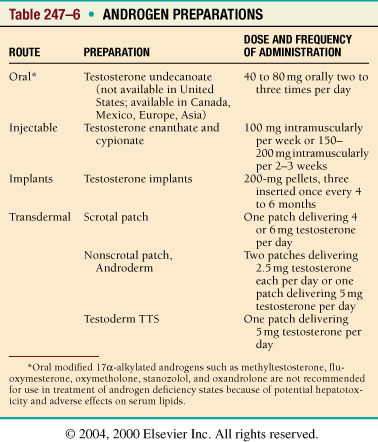
TESTOSTERONE/ANDROGEN
PREPARATIONS:
MONITORING THE EFFECTS OF TESTOSTERONE TREATMENT — Patients who are treated with testosterone should be monitored to determine that normal serum testosterone concentrations are being achieved. The serum testosterone should be measured midway between injections in men who are receiving testosterone enanthate, and the value should be mid-normal, eg, 600 to 700 ng/dL (20.8 to 24.3 nmol/L). The dose should be reduced if higher values are obtained. The serum testosterone can be measured at any time in men who are using any of the transdermal preparations, with the recognition that the peak values occur three to five hours after application of the scrotal patch and six to eight hours after application of the nonscrotal patch. The concentrations fluctuate when the gel is used, but not in a predictable way, so at least two measurements should be made at any dose of gel; the time of measurement does not appear to matter. The value should be well within the normal range (400 to 800 ng/dL [13.9 to 27.7 nmol/L]). If the patient has primary hypogonadism, normalization of the serum LH concentration should also be used to judge the adequacy of the testosterone dose, no matter which testosterone preparation is used. Desirable effects — Normalization of the serum testosterone concentration should lead to normal virilization in men who are not virilized and maintenance of virilization in those who already are. Men who become hypogonadal in adulthood and are still normally virilized, but whose hypogonadism is manifested by a decrease in libido and energy, should note a marked improvement in these symptoms. Failure of improvement when the serum testosterone concentration has been restored to normal suggests another cause of the symptoms. Testosterone replacement also leads to substantial improvements in muscle strength and bone density. In one report, for example, the administration of 100 mg of testosterone enanthate once a week for ten weeks to hypogonadal men increased their strength in the bench press by 22 percent and their squat strength by 45 percent. In another series, the effect of testosterone replacement on bone density was assessed in 72 hypogonadal men. The increase in bone density averaged 39 percent in the first year of testosterone replacement and eventually reached and was maintained in the normal range. The response was greatest in the first year in previously untreated patients and was most pronounced in those with lowest bone density measurements at baseline. Undesirable effects — Testosterone enanthate and the testosterone patch and gels have virtually no side effects unrelated to the action of testosterone. Testosterone enanthate rarely leads to infection at the injection site, while the scrotal patch occasionally leads to mild to moderate scrotal itching, which remits spontaneously or after the application of hydrocortisone cream. The patch, Androderm, often causes skin rashes, some very mild and others quite severe, requiring discontinuation of this treatment. The rash may sometimes be prevented by pretreatment of the skin with a corticosteroid cream. However, some of the actions of testosterone itself, while not side effects, are undesirable.
There is no reason to think that men who rely on medication to maintain a
normal serum testosterone concentration are more likely to develop these
conditions than men who produce their own testosterone.
RECOMMENDATIONS Men who begin using a transdermal preparation need to be seen two to three months after the initiation of therapy to measure the serum testosterone concentration and evaluate the possibility of undesirable effects. Men who use the body patch or a 50 mg dose of the gel, but whose serum testosterone concentration is not high enough, can try wearing two patches or applying 75 or 100 mg of the gel. The initial regimen of testosterone enanthate should be 200 mg IM every two weeks, which can be administered either by someone in the patient's household or by the patient himself. The patient should be seen approximately two to three months later and, if he is bothered by fluctuations in energy, mood, or libido, the regimen can be changed to 100 mg once a week or transdermal testosterone can be offered again.
|
| Primary
Hypogonadism | Secondary
Hypogonadism | Rx of Hypogonadism |
|
| Klinefelter’s syndrome is a congenital disorder in which an extra X chromosome 47, XXY chromosome complement is associated with hypogonadism and infertility, but greater and lesser numbers of X chromosomes have also been reported, resulting in karyotypes such as 48 XXXY and 46,XY/46,XXY mosaicism. 46,XX males also have Klinefelter's syndrome; the development of testes in this setting is presumably due to translocation of a small portion of chromosomal material containing the testis-determining factor to an X chromosome. Diagnosis of Klinefelter's syndrome usually can be made by determining the karyotype of the peripheral leukocytes. Testosterone deficiency and the resulting hypogonadism, if present, can be treated with testosterone. Hormone replacement is unlikely to improve the other abnormalities. INCIDENCE: 1 in 1000 men (most common sex chromosome disorder causing primary hypogonadism) GENETICS: The most common mosaic complement is 46,XY/47,XXY. 47,XXY karyotype and occasional 48,XXYY; 48,XXXY; or 49,XXXXY have been reported. The manifestations vary in severity in patients. It is this sex chromosome mosaicism that is thought to account for the variable presentation. Fertility, although very rare, has been reported in men with Klinefelter’s syndrome. PHYSICAL FINDINGS CLASSIC TRIAD: Small firm testes, azoospermia, and gynecomastia (others: infertility tall long legs) Postpubertal: Gynecomastia (periductal fat growth) with small, firm, pea-sized testes. Exaggerated growth of the lower extremities results in a decreased crown-to-pubis:pubis-to-floor ratio There are diminished strength, diminished ability to grow a full beard or mustache, infertility; decreased intellectual development and antisocial behavior are thought to occur with high frequency. LABORATORY TESTS
|
| Cryptorchidism
Cryptorchidism refers to one or both testes that are undescended; specifically, to testes that are in the abdominal cavity or in the inguinal canal and cannot be manipulated manually to within the scrotum by the age of one year. In comparison, testes that can be manipulated manually into the scrotum are called retractile. The etiology of cryptorchidism is unknown in most cases, but gonadotropin deficiency in utero appears to be one cause, as evidenced by the frequency of cryptorchidism in association with congenital hypogonadotropic hypogonadism. Some clinical consequences of cryptorchidism depend upon whether one or both testes are cryptorchid:
Another clinical consequence of a cryptorchid testis is an approximately 3- to 14-fold increased risk of testicular cancer. Treatment of cryptorchidism is designed to minimize heat-induced testicular damage by moving the cryptorchid testis into the scrotum, as well as to reduce the risk of malignancy and make the testis easier to palpate.
|
| Varicocele Varicosity of the venous plexus within the scrotum, called a varicocele, has long been considered a possible cause of damage to the seminiferous tubules and thereby of infertility. As a result, ligation of varicoceles has long been practiced as a treatment for infertile men. The proposed mechanism by which a varicocele damages the seminiferous tubules is increased blood flow, which raises the testicular temperature. However, infertile men who do not have a varicocele have scrotal temperatures similar to those in infertile men who have a varicocele. Many series have reported an improvement in semen qualities following varicocele ligation, but these studies were uncontrolled. Controlled trials have not demonstrated improvement in sperm count or fertility after varicocele correction. As a result, we cannot conclude that a varicocele impairs spermatogenesis or that correcting it will improve spermatogenesis.
|
| Primary Hypogonadism | Secondary Hypogonadism | Rx of Hypogonadism | |
![]()
![]() 2011
2011
Screening and Workup for Testosterone Deficiency
Martin M. Miner, MD
Medscape CME Released: 09/21/2011; Valid for credit through 09/21/2012
This program is jointly sponsored by New York Medical College and Continuing
Education Alliance.
Introduction
Estimates of the prevalence of testosterone deficiency (TD) in men vary widely, from 2.8% in community-dwelling men to 39% in men in patient populations.[1-3] Going by the higher estimate, which is based on biochemical evidence of TD, roughly 14 million men =45 years of age who visit a primary care provider (PCP) each year may be testosterone deficient.[2] Not all men with biochemical TD also have hypogonadal symptoms. Many do, however, have nonspecific, nonsexual symptoms that may suggest TD. Therein lies a major obstacle to identifying men with TD in primary care. A multitude of comorbidities have been found in conjunction with TD in prevalence studies—comorbidities seen with great frequency in primary care, including metabolic syndrome and diabetes, cardiovascular disease and hypertension, chronic inflammatory states including autoimmune diseases and chronic obstructive pulmonary disease (COPD), and long-term opiate use. The role of low testosterone as a cause or marker of these comorbidities is not clear, but as research continues to explore the question, the associations themselves mandate increased awareness of TD symptoms and clinician confidence in the screening and workup of at-risk patients.
Understanding Pathophysiology
Most patients who are experiencing TD want to know why they have the condition and where it originated. Although it is sometimes possible for the clinician to arrive at a definitive etiology of individual cases, more often the cause is multifactorial and complex.[4,5] The possible sites of origin are the testes, where testosterone is produced; and the brain, where the production process is regulated by means of the hypothalamic-pituitary-gonadal (HPG) axis. These 2 sites are the basis of a general classification scheme for TD in which hypogonadism is considered primary if it is testicular in origin and secondary if it results from hypothalamic or pituitary dysfunction (Table 1).[4,6] Each type of hypogonadism can be inherited or acquired, and each type can occur in men of any age.[7] However, most cases of hypogonadism in men aged 30 to 50 years are a mixed form, involving testicular failure as well as central defects of the HPG axis.[4,6,7] This form corresponds to what is often called adult-onset or late-onset hypogonadism (LOH).[5]
Table 1. Primary and Secondary Forms of Hypogonadism [4,6,8-10]
• Primary hypogonadism (testicular dysfunction)
• Secondary hypogonadism (hypothalamic or pituitary dysfunction)
• Mixed hypogonadism (seen chiefly in men aged 30 to 50 years old)
Relatively few cases of TD are primary; those that occur are usually congenital in origin, such as Klinefelter syndrome, the most common primary form.[4] Other primary causes include mumps orchitis, cryptorchidism, chemotherapy/radiation therapy, and testicular trauma.[6]
Causes of secondary hypogonadism include hypothalamic or pituitary lesions, cranial trauma, hyperprolactinemia, and Kallmann syndrome (genetic). Aging, acute illnesses, certain medications, and chronic illnesses including alcoholism, diabetes, cardiovascular disease, and sickle cell disease are believed to play causative roles in mixed hypogonadism.[6,10]
Although all forms of hypogonadism involve TD, they differ somewhat in their characteristic gonadotropin profiles. Primary hypogonadism is marked by increased luteinizing hormone (LH) and follicle-stimulating hormone (FSH), the result of reduced feedback from testosterone; secondary hypogonadism is characterized by low or low-normal levels of LH and FSH; and the mixed form varies according to the predominance of primary or secondary hypogonadism. All forms also involve impaired spermatogenesis.[7,11] The clinical guidelines of the Endocrine Society recommend measurement of LH and FSH in hypogonadal men to distinguish between primary and secondary hypogonadism.[11] A more rational approach is to reserve FSH measurement for hypogonadal patients who have fertility concerns. LH is directly relevant to testosterone production and, in the absence of fertility questions, is the only gonadotropin of interest for TD classification. Measurement of serum prolactin, for insight on pituitary function, is appropriate when the serum testosterone level is <150 ng/dL or when secondary hypogonadism is suspected.[12]
Identifying Candidates for Screening
Signs and symptoms typical of TD do not figure into the hypogonadism classification scheme because they do not distinguish one form from another; symptoms can be similar regardless of the etiology of TD. Nonetheless, both symptoms and biochemical evidence of hypogonadism are prerequisites for the diagnosis and treatment of TD. This principle presents the core challenge to clinicians, because the symptoms of TD are not specific to hypogonadism, and can, at best, raise suspicion of TD when they are present.
Hypogonadism symptoms
develop slowly and overlap with the symptom profiles of conditions such as
depression, erectile dysfunction (ED), and normal aging. They may
manifest as reduced libido, muscle mass, strength, and bone mass;
or as increases in mood disturbances, body fat, and hot flashes, all
of which can arise from causes other than TD. Their lack of specificity means
that these symptoms require corroboration by testosterone measurement, and
even a repeat measurement (ie, 2 low values), for final confirmation.[11,12]
As noted in the first Expert Column in this series on TD,[13] there is lack of agreement on the relevance of TD to ED, that is, whether ED is sufficiently symptomatic of hypogonadism to prompt screening and testosterone measurement. The Endocrine Society guidelines[11] do not specify ED as suggestive of TD. The American College of Physicians does not recommend for or against routine hormonal blood tests or hormonal treatment for ED, citing the wide-ranging prevalence rates of ED in hypogonadal men (12.5%-35%) and the lack of conclusive evidence about the impact of testosterone therapy on ED.[14,15] On the other hand, several other international medical societies[12] recognize ED as among the hallmark symptoms of TD requiring biochemical corroboration. Most primary care practitioners will know from their own experience that ED is the portal to testosterone measurement. It should by no means go unappreciated as a possible manifestation of TD.
National and international guidelines concur in recommending TD screening for men deemed at risk due to coexisting illnesses (Table 2). The conditions include infertility, type 2 diabetes, metabolic syndrome, chronic obstructive pulmonary disease, inflammatory arthritis, cardiovascular disease, and chronic use of glucocorticoids and opioids.[8,9,11,12] Clinicians should maintain a high index of suspicion of TD in patients with these comorbidities. Even those at-risk patients who report no symptoms typical of hypogonadism require a thorough clinical and biochemical workup for TD.
Table 2. Conditions With a High Prevalence of Testosterone Deficiency and Requiring Measurement of Serum Testosterone [5,11,12]*
*For men with sellar mass, HIV-associated weight loss, low-trauma fracture, or use of medications that affect testosterone production, measurement of testosterone should be considered regardless of hypogonadal symptoms.
There is little support for the use of formal questionnaires as a screening method for TD, especially as an isolated method in the workup. The Aging Males' Symptoms and the Androgen Deficiency in Aging Men scales, 2 of the better known symptom inventories used in TD screening, demonstrate high sensitivity for identifying men with TD but very low specificity (<40%),[16,17] making them unreliable for screening. In a recent trial with 587 community-dwelling men aged 60 to 80 years with known TD, the scores from these scales correlated more closely with age than with testosterone, and they did not reflect changes in symptoms after a 6-month regimen of testosterone therapy.[16] This latter finding is unfortunate because some clinicians find the instruments useful as a reference for evaluating the effects of treatments.[9]
However, the screeners may be helpful in identifying patients with a high likelihood of TD, and for educating the clinician about high-yield questions to ask in the TD workup. Even so, the current array of questionnaires are too time-consuming for most primary care clinicians to use routinely, especially given the lineup of other screeners suggested for primary care (for depression, dementia, and cancer, to name a few) that compete for time and resources. Newer screeners for TD are in development with fewer questions, and thus shorter completion time; these are likely to become available in the next 2 years.
Signs and Symptoms
Practice guidelines suggest that clinicians measure or consider measuring the testosterone levels of men who manifest any of these symptoms.[11,12] Another practical way to look at TD symptoms is from the perspective of affected domains (Table 3),[18] the 3 chief domains being sexual; psychological, including sleep; and physiologic, relating to strength, muscle mass, visceral obesity, and mobility. However symptoms are approached, clinicians should be aware that most of our current knowledge of TD symptoms is derived from clinical observations, and their own clinical judgment will be their chief resource as they proceed with the workup of TD. Symptoms may be vague: a general lack of energy, loss of motivation, inability to concentrate, a cantankerous mood, muscular aches.[4] The symptoms will also be affected by patient age, comorbid illnesses, the severity and duration of TD, previous testosterone therapy, and genetic factors.[9,11] The concern is that clinicians will connect these symptoms to aging or chronic disease or unhealthy lifestyle, and fail to investigate them as part of hypogonadism.
Table 3. Domains and Clinical Manifestations of TD in Men [8,11,12,18]
Sexual Domain
Psychological Domoain
Physiological Domain
In addition to testosterone measurement, the workup for hypogonadism should proceed with the patient's personal and family medical history and a physical examination that covers blood pressure, secondary sexual characteristics (body hair, beard, pubic hair), testicular examination, and measurement of waist circumference and fat distribution. Examination of the prostate is appropriate to assess prostate cancer (which will affect the decision and timing about testosterone repletion); a nonpalpable or small prostate suggests low testosterone. Small testes (<15 mL) suggest TD. Supplementary tests may be necessary to exclude conditions in the differential diagnosis of TD; for example, a bone density test for suspected osteoporosis, or magnetic resonance imaging (MRI) to detect a pituitary macroadenoma in men (especially those <50 years of age) with both low testosterone and low LH, or elevated prolactin. Older men with secondary hypogonadism should undergo MRI if their serum testosterone is very low (<150 ng/dL) and if LH is normal or low or prolactin is increased. Visual changes or headache should also prompt MRI scanning. Other conditions in the differential diagnosis of TD include diabetes insipidus, hypothyroidism, adrenocorticotropic deficiency, or acute infection. The clinician should also be vigilant regarding obstructive sleep apnea, which has been associated with TD as well as testosterone repletion and may require evaluation both before and after initiation of repletion therapy.[4,8]
Comorbidities Associated With TD
The links between TD and other illnesses are still being explored at all levels, but epidemiologic research has by now established several critical associations. The strongest links relate to diabetes and metabolic syndrome. The cross-sectional Hypogonadism In Males (HIM) study reported several years ago that TD occurs frequently in men with type 2 diabetes in a primary care population; these men had more than twice the risk of hypogonadism than men without diabetes.[2] A more recent HIM analysis, based on free-testosterone measurement in more than 1800 men, found that the hormone's concentration in obese men with diabetes was significantly lower than in obese men without diabetes. Forty percent of the men without diabetes in the population and 50% of the men (=45 years) with diabetes were testosterone deficient. In a decade's time, the average decline in free testosterone was 7.8 pg/mL in the men without diabetes and 8.4 pg/mL in men with diabetes. The HIM investigators proposed that obesity and diabetes (in addition to age) exert independent effects on the prevalence of TD, with obesity perhaps the most closely associated comorbidity; and that the presence of either obesity or diabetes in a patient should prompt measurement of testosterone, especially if they occur together.[19] Furthermore, diabetes should be considered as a potential comorbidity in men with ED or with diminished libido, whether or not TD is also present.[12]
Obesity is but one component of the metabolic syndrome, which also includes hypertension, dyslipidemia, impaired glucose regulation, and insulin resistance, to show a close relationship with TD. In a population of 794 community-dwelling men aged 50 to 91 years who were prospectively followed for 20 years in the Rancho Bernardo Study, low testosterone levels were associated with central obesity, hyperinsulinemia, insulin resistance, hyperglycemia, dyslipidemia, hypertension, and other cardiovascular risk factors such as low adiponectin and elevated C-reactive protein. Surprisingly, TD maintained an independent association with increased mortality during follow-up: men with total testosterone levels in the lowest quartile (<241 ng/dL) were 40% more likely to die than the men with higher levels, regardless of age, adiposity, and other components of the metabolic syndrome and cardiovascular risk. The excess mortality was mainly due to cardiovascular and respiratory diseases, and the authors theorized that obesity could be a pathway by which TD influences and promotes these problems.[20]
A recent review of research on the links between hypogonadism, metabolic syndrome, and cardiovascular disease concluded that any connections remain clinically and pathophysiologically unclear.[21] Other findings suggest meaningful associations. In a randomized trial of 32 hypogonadal men with metabolic syndrome and newly diagnosed type 2 diabetes, the men who received testosterone repletion in addition to lifestyle therapy experienced greater improvement in components of the metabolic syndrome, with more than 80% of these men achieving reversal of syndrome parameters and reaching all specified targets for glycemic control.[22,23] In addition, a double-blind, placebo-controlled trial involving 50 men with metabolic syndrome found that testosterone therapy significantly reduced insulin resistance and C-reactive protein. Testosterone therapy was also credited with delaying the progression of atherosclerosis as assessed by intima-media thickness of the carotid artery.[24] Continued focus on the relationships between TD, metabolic disorders, and cardiovascular disease is an important research objective.
TD is one of numerous hormonal disorders associated with HIV and acquired immunodeficiency syndrome (AIDS), although its prevalence and pathogenesis have changed in the past 20 years. Originally associated with advanced AIDS, particularly wasting syndrome, hypogonadism is now less prevalent in the HIV/AIDS population and is now associated with aging, comorbidities (eg, hepatitis C), and drug side effects. There is no established connection between antiretrovirals and TD, but injection drug use and psychotropic medications are associated with TD in older men with HIV.[25] Drug use has also emerged as a comorbidity of TD in the general population. Given the known increase in both therapeutic and nonmedical uses of opioids in the past 10 years, it is not surprising that more men with a history of chronic use of these drugs (such as methadone, oxycodone, hydrocodone, morphine, and codeine) are presenting with associated complaints. Beyond the inherent risks of overuse and misuse, including death, the long-term effects of opioid medications are now believed to include hypogonadism, sexual dysfunction, and hyperalgesia.[26] Pituitary hormones may also be altered with continued use, and the risks of infertility and bone loss may rise (in men and women). Furthermore, opioids may increase or decrease food intake, cause hypoglycemia, and impair insulin secretion. This excessive stress is difficult for body systems to tolerate, so it is troubling that the rate of substance abuse has increased among adults aged 60 years and older, the aging baby boomers. Alcohol and prescription drug abuse may by now affect as many as 17% of older adults.[27]
Measuring Testosterone: What Do the Values Mean?
Total testosterone (TT) has been the traditional measure for use in corroboration of hypogonadism. Testosterone levels in healthy men follow a circadian rhythm, with levels peaking in the morning. Accordingly, guidelines recommend measurement of TT in a blood sample taken during morning hours, preferably after the patient has fasted. A positive finding should be repeated, especially if borderline.[9,11]
Values for "normal" testosterone vary among laboratories according to the assay in use. Even if assays were consistent, there is no clear clinically relevant dividing line between normal and deficient testosterone in the blood, despite the efforts of involved medical societies to define one (Table 4). It is generally agreed that a TT level of >350 ng/dL does not require treatment and suggests nontestosterone sources of symptoms. Otherwise, the recommendation is to consider treating men with "unequivocally low" testosterone along with symptoms. Clinicians should be aware that TT measurements do not necessarily correspond with the patient's clinical presentation. Some research supports symptom-specific levels of TT below which the prevalence of the symptom starts to increase.[28] Other research finds no symptom-specific thresholds but further evidence that the severity of symptoms increases with decreasing testosterone level, most clearly the severity of psychological symptoms.[29]
Table 4. Biochemical Definitions of Hypogonadism [8,11,12,30]
Total Testosterone Level
| Society Guidelines | ng/mL | ng/dL | nmol/L |
| EAA, ISA, ISSAM | < 3.40 | < 340 | < 12 (mild) |
| EAU, ASA, ISSM | < 2.31 | < 231 | < 8 (severe) |
| ES | < 3.00 | < 300 | < 10.4 |
| AACE | < 2.00 | < 200 | 7 |
EAA = European Academy of Andrology; ISA = International Society of Andrology; ISSAM = International Society for the Study of the Aging Male; EAU = European Association of Urology; ASA = American Society of Andrology; ISSM = International Society for Sexual Medicine; ES = Endocrine Society; AACE = American Association of Clinical Endocrinologists.
TT represents the total of free testosterone plus hormone bound to sex hormone-binding globulin (SHBG) and albumin. TT levels are subject to alterations in SHBG that occur in association with obesity, old age, diabetes, medications, and other confounders.[11] Measurement of free testosterone can be of diagnostic value in cases where TT does not correspond with the clinical picture. However, this practice is limited by the availability of assays and, again, a lack of consensus on threshold values. Many clinicians who regularly see men with TD suggest a threshold of 8 ng/dL to define hypogonadism by calculated free testosterone. For measurement by means of the analog free-testosterone assay, values <1.5 ng/dL have been proposed as a lower limit of normal.[18]
Our upcoming Expert Column will discuss the treatment of TD, which has already achieved successes in improving sexual symptoms, body composition and strength, bone density, and glycemic parameters, effects with an indisputable relevance to quality of life and overall good health.
This article is a CME certified activity. To earn credit for this activity
visit:
http://www.medscape.org/viewarticle/749240
References
Araujo AB, O'Donnell AB, Brambilla DJ, et al. Prevalence and incidence of androgen deficiency in middle-aged and older men: estimates from the Massachusetts Male Aging Study. J Clin Endocrinol Metab. 2004;89:5920-5926.
Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM Study. Int J Clin Pract. 2006;60:762-769.
Wu FC, Tajar A, Beynon JM, et al; EMAS Group. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363:123-135.
Miner MM, Sadovsky R. Evolving issues in male hypogonadism: evaluation, management, and related comorbidities. Cleve Clin J Med. 2007;74(suppl 3):S38-S46.
Corona G, Rastrelli G, Forti G, Maggi M. Update in testosterone therapy for men (CME). J Sex Med. 2011;8:639-654.
Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pract. 2010;64:682-696.
Bassil N, Morley JE. Late-life onset hypogonadism: a review. Clin Geriatr Med. 2010;26:197-222.
Petak SM, Nankin HR, Spark RF, Swerdloff RS, Rodriguez-Rigau LJ; American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for clinical practice for the evaluation and treatment of hypogonadism in adult male patients—2002 update. Endocr Pract. 2002;8:440-456.
Arver S, Lehtihet M. Current guidelines for the diagnosis of testosterone deficiency. Front Horm Res. 2009;37:5-20.
Swerdloff RS, Wang C. The testis and male sexual function. In: Goldman L, Ausiello DA, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2008:1782-1798.
Bhasin S, Cunningham GR, Hayes FJ, et al; Task Force, Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95:2536-2559.
Wang C, Nieschlag E, Swerdloff RS, et al. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Aging Male. 2009;12:5-12.
Miner MM. Low Testosterone Medscape CME Expert Column Series. Issue 1: Testosterone deficiency in men: common and under-recognized. 2011. Available at: http://www.medscape.org/viewarticle/746602. Accessed August 18, 2011.
Qaseem A, Snow V, Denberg TD, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Hormonal testing and pharmacologic treatment of erectile dysfunction: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2009;151:639-649.
Buvat J, Montorsi F, Maggi M, et al. Hypogonadal men nonresponders to the PDE5 inhibitor tadalafil benefit from normalization of testosterone levels with a 1% hydroalcoholic testosterone gel in the treatment of erectile dysfunction (TADTEST study). J Sex Med. 2011;8:284-293.
Emmelot-Vonk MH, Verhaar HJJ, Nakhai-Pour HR, Grobbee DE, van der Schouw YT. Low testosterone concentrations and the symptoms of testosterone deficiency according to the Androgen Deficiency in Ageing Males (ADAM) and Ageing Males' Symptoms rating scale (AMS) questionnaires. Clin Endocrinol (Oxf). 2011;74:488-494.
Morley JE, Perry HM III, Kevorkian RT, Patrick P. Comparison of screening questionnaires for the diagnosis of hypogonadism. Maturitas. 2006;20;53:424-429.
Traish AM, Miner MM, Morgentaler A, Zitzmann M. Testosterone deficiency. Am J Med. 2011;124:578-587.
Dhindsa S, Miller MG, McWhirter CL, et al. Testosterone concentrations in diabetic and nondiabetic obese men. Diabetes Care. 2010;33:1186-1192.
Laughlin GA, Barrett-Connor E, Bergstrom J. Low serum testosterone and mortality in older men. J Clin Endocrinol Metab. 2008;93:68-75.
Corona G, Rastrelli G, Morelli A, Vignozzi L, Mannucci E, Maggi M. Hypogonadism and metabolic syndrome. J Endocrinol Invest. [Epub ahead of print].
Heufelder AE, Saad F, Bunck MC, Gooren L. Fifty-two-week treatment with diet and exercise plus transdermal testosterone reverses the metabolic syndrome and improves glycemic control in men with newly diagnosed type 2 diabetes and subnormal plasma testosterone. J Androl. 2009;30:726-733.
Jones TH, Arver S, Behre HM, et al; TIMES2 Investigators. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study). Diabetes Care. 2011;34:828-837.
Aversa A, Bruzziches R, Francomano D, et al. Effects of testosterone undecanoate on cardiovascular risk factors and atherosclerosis in middle-aged men with late-onset hypogonadism and metabolic syndrome: results from a 24-month, randomized, double-blind, placebo-controlled study. J Sex Med. 2010;7:3495-3503.
Cotter AG, Powderly WG. Endocrine complications of human immunodeficiency virus infection: hypogonadism, bone disease and tenofovir-related toxicity. Best Pract Res Clin Endocrinol Metab. 2011;25:501-515.
Manchikanti L, Fellows B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician. 2010;13:401-435.
Vuong C, Van Uum SHM, O'Dell LE, Lutfy K, Friedman TC. The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr Rev. 2010;31:98-132.
Zitzmann M, Faber S, Nieschlag E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J Clin Endocrinol Metab. 2006;91:4335-4343.
Lackner JE, Rücklinger E, Schatzl G, Lunglmayr G, Kratzik CW. Are there symptom-specific testosterone thresholds in aging men? [published online ahead of print January 13, 2011]. BJU Int. [Epub ahead of print].
Buvat J, Maggi M, Gooren L, et al. Endocrine aspects of male sexual dysfunctions. J Sex Med. 2010;7:1627-1656.
{kind=link}
{kind=link}
{kind=link}