![]()
Contrast-induced Nephropathy
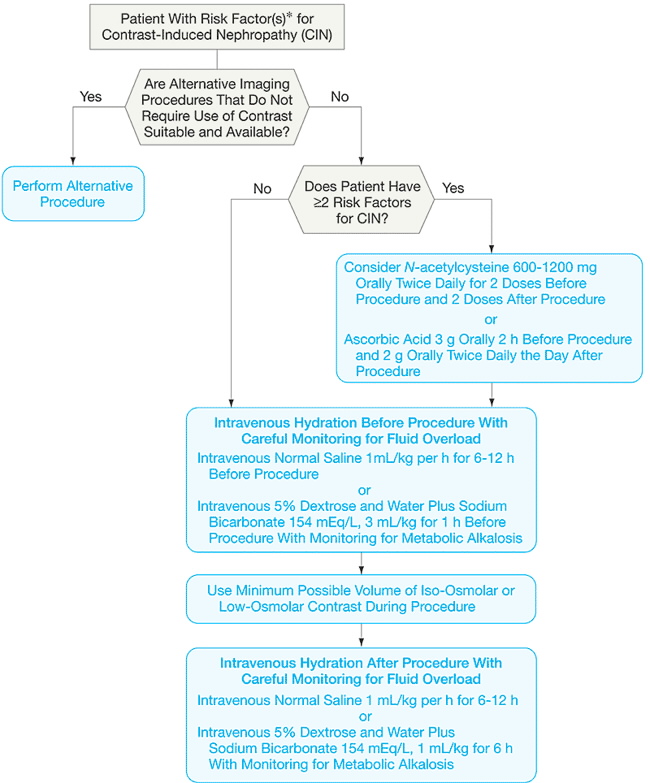
Contrast-induced Nephropathy | Strategy (figure)
REF: JAMA Volume 295(23), 21 June 2006, p 2765–2779
Two risk scores for contrast-induced nephropathy developed from large interventional cardiology databases may be the most generalizable to this patient population.
Bartholomew et al 16 (n = 20 479) identified 8 variables that were associated with contrast-induced nephropathy
and created 4 risk categories based on their analysis.
They defined contrast-induced nephropathy as a greater than 1 mg/dL [88.4 µmol/L] rise in SCr with no specified time frame for post SCr measurement. By this definition, contrast-induced nephropathy occurred in 2% of patients.
Patients in the highest risk group had a 28% risk of developing contrast nephropathy and a 17% risk of death.
Mehran and colleagues (n = 8357) identified 3 additional characteristics that were associated with increased risk:
They used a less stringent definition of contrast-induced nephropathy (change in SCr >=25% or >=0.5 mg/dL [44.2 µmol/L] at 48 hours), which may partially account for the higher reported incidence of contrast-induced nephropathy (13.1%).
Management to reduce contrast-induced nephropathy
![]()
![]()
06072003