BPH - Benign Prostate Hypertrophy
|
| REF:
bph2008.pdf
|
| Diagnosis
Include history, physical exam (with digital rectal exam), urinalysis, PSA,
and serum creatinine concentration in the diagnostic evaluation for suspected
BPH.
History and Physical Examination
-
Quantify symptom severity by using the American Urological Association Symptom
Index.
-
Because prostate size does not correlate with obstructive and irritative
symptoms, use information from the history taking to indicate the possible
presence of BPH.
-
Use digital rectal exam and focused neurologic exam to rule out other conditions
in patients with symptoms suggesting BPH.
LUTS (lower urinary tract symptoms) seen in BPH:
-
Storage type Sx:
-
Urgency, frequency, nocturia, urge incontinence, stress incontinence
-
Voiding type Sx:
-
hesitancy, poor flow, intermittency, straining, dysuria
-
Postmicturition type Sx:
-
terminal dribble, postvoid dribble, incomplete emptying
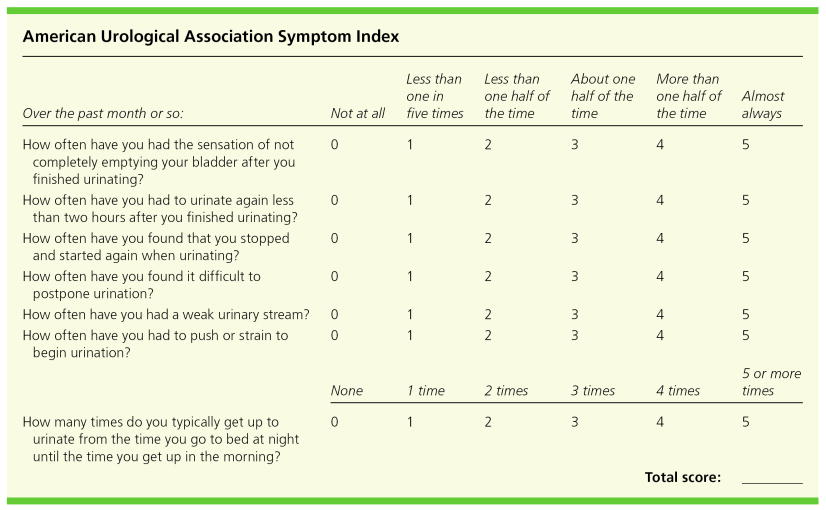
American Urological Association Symptom Index to
assess severity of benign prostatic hyperplasia (BPH)
See Figure: BPH AUA Symptom Index
A score of 7 or less indicates mild BPH; a score of 8 to 19 indicates
moderate BPH; a score of 20 to 35 indicates severe BPH.
Adapted with permission from American Urological Association. Guideline on
the management of benign prostatic hyperplasia (BPH).
http://www.auanet.org/guidelines/bph.cfm. Accessed September 19, 2007.
|
|
Laboratory Tests
-
Recognize that measuring serum PSA in patients with suspected BPH is
controversial.
-
Bladder Ultrasound to check for urinary retention
-
In & out cath to check for urinary retention
-
Renal sonogram to check for hydronephrosis - sign of urinary obstruction
|
|
Drug Treatment
of Benign Prostatic Hyperplasia
-
Include alpha 1 blockers, or 5-a-Reductase inhibitor, or a combination of
the two.
-
Encourage patients with mild BPH who are enthusiastic about
saw palmetto berry extract, or alternative
medicine in general, to try this form of therapy.
alpha 1 adrenegic blockers (* risk
of orthostatic hypotension)
-
Relaxation of prostatic smooth muscle and relief of the dynamic component
of bladder outlet obstruction.
-
Improved symptom scores and urinary flow rates
-
Use as first-line therapy for patients with BPH who have clinically significant
symptoms but are not experiencing urinary retention.
-
Side effects of alpha blockers include orthostatic hypotension, dizziness,
and asthenia. The last two side effects are not primarily mediated by low
blood pressure. Tamsulosin (Flomax) and alfuzosin (UroXatral) do not
affect blood pressure, as do the other alpha blockers; Abnormal ejaculation
has been reported in about 10% of men on tamsulosin.
-
Terazosin (Hytrin) start with 1 mg hs, max 20 mg
-
Initially 1 mg qhs; can be titrated up to 20 mg qd
-
Syncope, dizziness, orthostatic hypotension, nausea, edema, impotence
-
The most studied drug in this class. Use cautiously with other antihypertensives.
Titration should proceed on the basis of response to therapy and side effects
-
Prazosin (Minipress) start with 1 mg bid, max 5
mg tid
-
Monitor blood pressure. Use cautiously with other antihypertensives. Titration
should proceed on the basis of response to therapy and side effects
-
Syncope, dizziness, orthostatic hypotension
-
Doxazosin (Cardura) startwith 1 mg daily; max 8
mg
-
Initially 1 mg qhs; can be titrated up to 8 mg qd
-
Dizziness, fatigue, hypotension, edema, dyspnea
-
Monitor blood pressure. Avoid in patients with liver dysfunction. Titration
should proceed on the basis of response to therapy and side effects.
-
Silodosin (Rapaflo) 4 to 8 mg capsule
once daily
Selective alpha blockers (* no effect
on resting blood presssure; risk of orthostatic hyotension)
-
Tamsulosin (Flomax) 0.4 mg PO daily
-
Initially 0.4 mg qd; can be increased to 0.8 mg qd after 2 weeks if response
is inadequate
-
Dizziness, orthostatic hypotension, rhinitis, abnormal ejaculation, decreased
libido, insomnia
-
Use cautiously with cimetidine and warfarin. Titration should proceed on
the basis of response to therapy and side effects
-
Alfuzosin (UroXatral) 10 mg PO daily after a
meal
-
Postural hypotension, chest pain, priapism, dizziness, headache
5-a-Reductase inhibitor (5ARI) (*
6 months of Rx is needed to achieve Sx relief)
-
Decrease in prostate volume; by 12 months, the PSA is reduced by 50%, then
the PSA reduction plateaus at 50% of baseline.
Men who take finasteride at the recommended dose of 5 mg daily
or dutasteride at 0.5 mg daily can expect a 20%
to 25% reduction in prostate size over the first year of therapy,
accompanied by about a 50% reduction in PSA
level. Despite this effect on PSA, these drugs have not been shown
to impair the ability to diagnose prostate cancer in controlled trials. However,
PSA levels must be interpreted differently. The most common recommendation
is simply to double the measured PSA levels for men on finasteride or
dutasteride, then interpret the results as usual.
-
Reserve 5-a-reductase inhibitors for
patients with large prostates who remain symptomatic while taking a 1-blockers.
-
Improved symptom scores and urinary flow rates
-
Use as second-line therapy; most efficacious in men with the largest prostates
(>40 g)
-
Finasteride (Proscar) is relatively well tolerated. About
5% to 10% of men notice decreased libido or ejaculatory
abnormalities over the first year of treatment; fewer than 1%
of men have rashes, gynecomastia, or breast tenderness. After the first year
of treatment, side effects with finasteride and placebo are essentially
identical. The side-effect profile of dutasteride (Avodart) is similar.
-
Finasteride (Proscar) 5 mg daily PO
-
Impotence, ejaculate volume, decreased libido
-
Avoid in patients with liver dysfunction.
-
Titration should proceed on the basis of response to therapy and side effects
-
Dutasteride (Avodart) 0.5 mg daily PO
-
Avodart reduces the risk of acute urinary retention by 57% , and BPH-related
surgery by 48% at 2 years)
-
Impotence, ejaculate volume, decreased libido, gynecomastia
-
Use with caution in patients with hepatic dysfunction
|
|
| Surgical Treatment
Options for BPH
Transurethral resection of the prostate
(TURP) - the benchmark therapy for BPH
-
Gold standard to which all other surgical options are compared
-
Transurethral approach in which the prostate is scraped by a wire loop, which
shaves a channel through the prostatic urethra
-
Incidence of side effects varies according to patient age, comorbid illness,
and prostate size Successful 80% of the time
-
Perioperative complications: bleeding requiring transfusion (3%-5%), UTI,
dilutional hyponatremia from bladder irrigation (16)
-
Long-term side effects: erectile dysfunction (14%), retrograde ejaculation
(74%), urethral stricture, bladder neck contracture, incontinence (5%) (16;
22)
-
30-day mortality rate: 0.4% in patients age 65–69, 1.9% in patients
age 80-84 (23)
Open prostatectomy
-
Oldest and most invasive BPH treatment
-
Complication rate is highest compared with all other surgical options
(6.9%-42.7%) (3)
Transurethral incision of the prostate
-
Transurethral approach in which one or two cuts in the prostate and prostatic
capsule are made, thereby decreasing constriction of the urethra
-
Performed almost exclusively in patients with small glands (<30 g)
-
The procedure of choice for men in whom fertility and ejaculation are important
-
Associated with a 78%-83% chance of symptom improvement and causes less morbidity
than transurethral resection.
-
Postoperative retrograde ejaculation occurs in < 25% of patients
(3)
Transurethral incision of the prostate (TUIP) involves making
one or two longitudinal incisions in the prostate without resecting tissue.
This procedure has been considered especially well suited to younger men
with smaller prostates. In a meta-analysis of four small trials, symptom
relief at 12 months with TUIP was similar to that with TURP. However, long-term
comparative results are not available. The risk of retrograde ejaculation
was 73% with TURP but only 21% with TUIP.
Transurethral electrovaporation of the prostate
-
Transurethral approach in which the prostate is shaved with a grooved roller
electrode; high levels of electricity (electrode >100°C) vaporize
prostate tissue
-
Advantage over transurethral resection: Decreased bleeding, decreased need
for postoperative hospitalization and catheterization
Minimally invasive surgical therapies:
Transurethral needle ablation of the prostate
-
Low-level radiofrequency waves are delivered to the prostate cystoscopically
via needles that heat the prostate, leading to tissue necrosis and sloughing
-
Advantages: No anesthesia or hospitalization, negligible incontinence or
sexual dysfunction.
-
Symptomatic improvement is less than that with transurethral resection
Interstitial laser coagulation
-
Achieved by a similar cystoscopic approach to that used with transurethral
needle ablation
-
Contact method: tissue vaporization immediately relieves the obstruction
but is technically difficult and time consuming
-
Noncontact method: creates coagulation necrosis by delivering laser energy
into the tissues that causes delayed tissue sloughing; as a result, a catheter
must be left in place longer
-
Because lasers have excellent hemostatic properties, this procedure may be
a good choice for patients taking anticoagulants or those with coagulation
disorders
-
Longer-term trials comparing visual laser ablation
of the prostate (VLAP) and contact laser
vaporization with TURP have also shown higher retreatment rates
with the laser strategies over 3 to 5 years.
Transurethral microwave thermotherapy of the prostate
(TUMT)
-
Direct heating of prostatic tissue by high energy (which is superior to low
energy).
-
The high-energy method is more painful than the low-energy method, necessitating
sedation and anesthesia.
-
This technique results in urethral irritation and a possibly prolonged
catheterization
-
Efficacy of this approach varies widely across studies
-
TUMT reduced symptoms more than terazosin in an 18-month trial; however,
in small trials comparing TUMT and TURP, symptomatic outcomes were somewhat
less impressive with TUMT. One long-term trial suggested that TUMT and TURP
yielded similar results at 5 years, a conclusion limited by the dropout of
a third of subjects.77 TUMT produces fewer side effects related to bleeding
than does TURP.
Management of Acute Urinary Retention
Acute urinary retention occurs at a rate of 1% to 2% a year in men with LUTS
attributable to BPH. The occurrence of acute urinary retention used to be
considered an absolute indication for surgery. However, case series have
documented that up to half of men with acute retention have a successful
voiding trial after a period of catheter
drainage, and most of the men who experience success will continue
to void, at least over a 6 month period following the procedure. The optimal
duration of catheter drainage is poorly defined, with recommended periods
ranging from a few days to several weeks.


|
|
The Long-Term Effect of Doxazosin,
Finasteride, and Combination Therapy on the Clinical Progression of Benign
Prostatic Hyperplasia
NEJM
Volume 349:2387-2398 December 18, 2003 Number 25
John D. McConnell, M.D, etc.
Result: The risk of overall clinical progression — defined as
an increase above base line of at least 4 points in the American Urological
Association symptom score, acute urinary retention, urinary incontinence,
renal insufficiency, or recurrent urinary tract infection — was
significantly reduced by doxazosin (39 percent risk reduction) and finasteride
(34 percent risk reduction), as compared with placebo.
The reduction in risk associated with combination
therapy (66 percent for the comparison with placebo) was significantly
greater than that associated with doxazosin or finasteride alone. The risks
of acute urinary retention and the need for invasive therapy were significantly
reduced by combination therapy and finasteride but not by doxazosin. Doxazosin,
finasteride, and combination therapy each resulted in significant improvement
in symptom scores, with combination therapy being superior to both doxazosin
and finasteride alone. [The dose of finasteride was 5 mg. The
dose of doxazosin was doubled at one-week intervals, beginning with 1 mg
daily for the first week, until the final daily dose of 8 mg was reached.]
Conclusions: Long-term combination therapy
with doxazosin and finasteride was safe and reduced the risk of overall clinical
progression of benign prostatic hyperplasia significantly more than did treatment
with either drug alone. Combination therapy and finasteride alone
reduced the long-term risk of acute urinary retention and the need for invasive
therapy.
2008
|
|
Medications &
Medical Conditions That May Contribute to LUTS (lower urinary tract symptoms)
in Men
REF: www.aafp.org/afp May 15, 2008 BPH article
-
Antihistamines - decreased parasympathetic tone
-
Decongestants - increased sphincter tone via alpha1-adrenergic receptor
stimulation
-
Diuretics - increased urine production
-
Opiates - impaired autonomic functin
-
Tricyclinc antidepressants - anticholinergic effects
-
Prostatitis
-
Prostate or Bladder cancer
-
Congestive heart failure - diuresis
-
Diabetes - osmotic diuresis, autonomic neuropathy (neurogenic bladder)
-
Parkinson's disease - autonomic neuropathy
|
|
|
|
|
|
|
|
|
|
|
|
{kind=link}